


Post-pregnancy Repair of Diastasis Recti
What is Diastasis Recti?
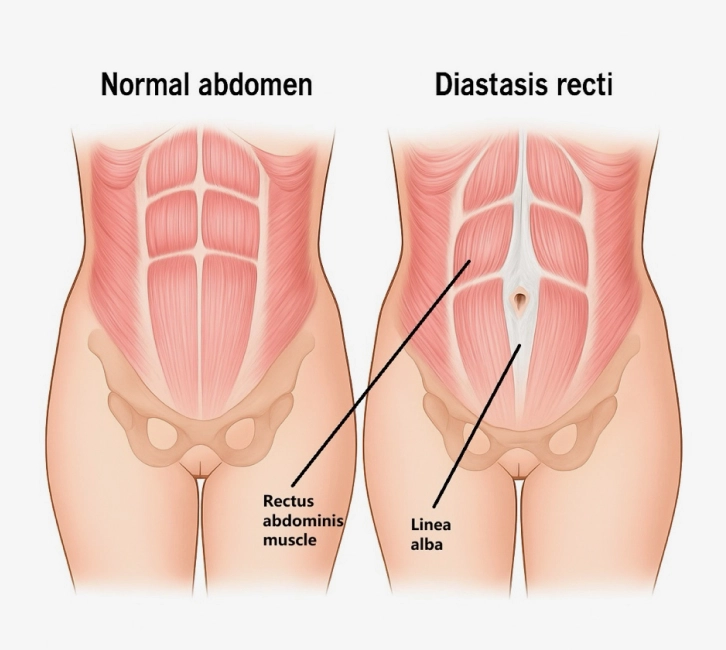
The word "diastasis" comes from the Greek word diástasis which means "separation" or "standing apart" and the word “recti” refers to the 2 abdominis recti muscles running vertically along the middle of your tummy, from the sternum to the pubic bone.
In medical terms, “diastasis” refers to an abnormal separation of normally joined parts, and in the context of pregnancy and post child-birth – “diastasis recti” refers to the separation of the rectus abdominis muscles.
Is Diastasis Recti common?
Using over 2cm separation as a criterion, there are some studies which show at 1 year post child-birth, approximately 33% women still have diastasis of recti, that means, approximately 1/3 women continue to have muscle separation which did not return to its original position. Along-side the diastasis, many women also have a lot of excess skin resulting from the expansion of their tummy during pregnancy, and often-times, after child-birth, this skin does not contract back to pre-pregnancy state. This explains why despite exercise and dieting after pregnancy, some women persistently have a “big tummy”.
Why does Diastasis Recti happen after pregnancy?
As your baby grows in your womb, the uterus expands and pushes against your abdominal muscles which causes separation of the abdominis rectus muscles and also stretches the tummy skin. Another effect the expanding womb has is to tent the diaphragm and cause the ribs to flare outwards, also known as “rib flaring”. This can sometimes cause pain as the ribs are pushed outwards.
Factors which make it harder for Diastasis Recti to recover:
- Big or heavy baby
- Having multiples (twins or triplets)
- Multiple pregnancies
- Improper abdominal binding after child-birth
- Poor muscle strength before getting pregnant. Research indicates that regular exercise before pregnancy appears to reduce the risk of diastasis recti and narrows the separation distance between the muscles. Strong muscles are better able to spring back together versus weak muscle.
- Possibly age, but an older yoga or Pilates instructor would probably have better chance of muscle recovery than a more sedentary younger woman.
- Higher amount of visceral fat as this intra-abdominal fat also plays a part in how much pressure is exerted against the abdominal muscles.

How do mums know if they have Diastasis Recti?
As most women may be nervous about pressing into their own tummy, if you suspect you have diastasis, it is best to have a medical/health-care professional perform a thorough physical examination and examine the extent of how wide apart your recti muscles are from each other.

It can be measured in finger widths, for example two to four fingers’ separation of the edges of rectus abdominis muscles

- the width of diastasis
- thickness of peripheral fat (fat between skin and muscle)
- thickness of rectus abdominis muscle - thinner muscles are usually weaker, thicker muscles are usually stronger, this information can give us a general idea of your abdominal muscle strength.
Symptoms of Diastasis
- Persistent abdominal bulge that does not improve with time or exercise
- Tummy shape is particularly round and looks like it is sticking out and unusually disproportionate compared to pre-pregnancy.
- Softness or jelly-like feeling around belly button
- Poor muscle strength can lead to poor posture.
“With my mummy patients, I particularly enjoy seeing their “ah ha” moment when I explain to them what diastasis recti is, and it is nothing they did or did not do which caused the diastasis.”
Diastasis Recti Treatment
Your plastic surgeon will do an abdominal examination and usually advise you to have a CT scan of the abdomen to accurately assess the extent of diastasis and check for hernias. He or she will then plan your surgery with you which is usually repairing the diastasis along with removing excess skin and fat i.e. tummy-tuck and repair of diastasis recti.

What kind of results can mums expect after treatment?
Post surgery, the contour of the abdomen is flatter than before and the belly-button will appear more normal.
The scar depends on the procedure performed.
- Traditional tummy-tuck and repair of diastasis:
Incision/scar will be hip-to-hip along the pubic region. Can be hidden under regular underwear, swim suits and non-string bikinis. - Minimally-invasive tummy tuck for patients with very little excess skin and fat:
2–3 short incisions in the abdomen for laparoscopic repair of diastasis and abdominal liposuction.
How long is the recovery process, and can mums still carry out their daily duties?
Post surgery, patients will be given strong and adequate pain-killers. It is rare for patients to be in pain. Most patients who had a previous C-section describe the recovery from a tummy-tuck to be better and more comfortable than the C-section. Probably because you do not have to care for a baby after this surgery and there is no uterus contraction pain. You can focus totally on your own recovery. Patients are welcome to stay as long as they like in hospital or whenever they feel ready to go home, but on average, most patients stay in hospital for 2-4 days.

Post traditional tummy-tuck and repair of diastasis
- Patients will step down from the bed with the assistance of a physiotherapist and sit on a chair or stand at bed-side. If the patient is feeling up to it, the physiotherapist will assist with walking. For the first few days, walking is usually a little bit hunched over to avoid stressing the abdominal incision.
- Urine catheter can be removed.
- Donning of compression garment by surgeon/nurse.
- Patients are able to stand straight and lie completely flat in bed.
- Most can go back to work after 2–3 weeks.
- Compression garments are usually worn for up to 1-month post-surgery.
Have questions about procedure details? Our team is here to help you every step of the way.
Connect with usFAQs on Diastasis Recti
Abdominal crunches can worsen the diastasis if done too early. While your muscles are trying to heal and get back to its original position, abdominal crunches done too early may have the opposite effect and push them further apart. It is best to see a post-partum physiotherapist early to examine and advise the best form of exercises and muscle therapy depending on the stage of post child-birth you are at.
Using the hammock again as an analogy. Now there is a hole in this hammock, and this person’s elbow gets stuck through this hole. Again, the person lying on the hammock is your abdominal contents and visceral fat. This situation is called a hernia as some of your abdominal contents is actually passing through this hole. And there is a “neck” where the contents are passing through the hole which can, in some cases, strangulate the hernia.
Small umbilical (belly-button) hernias can be common in post-pregnancy women, and are usually an aesthetic problem. But umbilical hernias can rarely become strangulated and this is an urgent medical issue.
A worsening and widening of diastasis of recti can lead to a hernia which can pose both aesthetic and functional problems. I have a patient who is very slim but has a belly that sticks out causing her T-shirt to ride up. When I took a history, she told me her last baby was very big and was also low-lying. I sent her to have a CT abdomen which confirmed a very wide diastasis with some herniation of a loop of colon. I repaired this hernia and removed a lot of excess skin to restore her flat tummy.
As for the down-time, the most common situation my patients compare their surgery with is to a C-section and they all say it is better than recovering from the C-section, as there is no newborn to look after, no uterus contraction pain, husbands or home carers are primed to look after the kids and manage the chores so patients can focus on recovery. Patients are back to using their phones and lap-tops Day 1 post-surgery and are usually in a good mood as they take the few days in hospital as an opportunity for a break.
“It was after becoming a mother myself, that I had a more personal perspective on body contouring post child-birth. And in a way, I also felt a certain kinship with my mummy patients.”
Consultation and Clinic-based Procedures:
101 Irrawaddy Road, #17-08
Royal Square Medical Centre
Singapore 329565
Consultation:
6 Napier Rd, #05-03
Gleneagles Medical Centre,
Singapore 258499
Contact Information:
Tel : +65 6592 7880
WhatsApp : +65 9831 8618
Operating Hours: